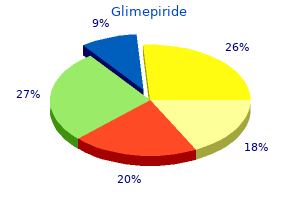
Glimepiride"Glimepiride 1mg with amex, diabetes medications guidelines". By: S. Lukjan, M.S., Ph.D. Clinical Director, UAMS College of Medicine The brain of a 63-year-old female patient diabetes medications without side effects discount 1mg glimepiride with visa, who had presented with adult-onset migrainous headache with visual aura and who had her first stroke at the age of 52 years. Thereafter, strokes recurred several times per year and she became demented, with other stroke-related deficits. There are multiple subcortical infarcts, most obvious in the deep grey matter and left parasagittal frontal white matter. These methods are practical when diagnosing new families with suspected disease, because genetic screening can be labour intensive and costly. The predominantly normotensive patients, generally from families with consanguinity, have severe non-amyloid arteriopathy, leukoencephalopathy and lacunar infarcts together with characteristic spinal anomalies and alopecia. In vitro studies suggested that apart Small Vessel Diseases of the Brain 171 2 Transcription Gene expression and/or repression. The putative Notch signalling pathway involves a complex series of proteolytic cleavage events eventually mediating transcriptional activation of a target gene. The following recruitment of the coactivator, Maml (mastermind-like), promotes transcriptional activity of its target genes, such as the hairy/enhancer of split (Hes). Diagram redrawn courtesy of Y Yamamoto, Yamaguchi University Graduate School of Medicine, Japan. Patients also have orthopaedic manifestations, including intervertebral disc herniations, kyphosis, ossification of spinal ligaments and various osseous deformities. Multiple small foci of softening and cavitation are seen in the cerebral white matter, basal ganglia, thalamus and brain stem. The intima shows marked fibrous thickening and the internal elastica is fragmented. Vascular smooth muscle cells in the media are destroyed and adventitia is thinned. Degeneration of both the medial and adventitial 172 Chapter 2 Vascular Disease, Hypoxia and Related Conditions layers is likely to impair autoregulation and functional hyperaemia. Diagram courtesy of Y Yamamoto, Yamaguchi University Graduate School of Medicine, Japan. The retinal microvessels undergo progressive occlusion leading to ischaemic retinopathy with subsequent optic disc atrophy and formation of capillary aneurysms. Pathological changes include foci of necrosis in the white matter, with prominent perivascular inflammation, oedema and astrocytic gliosis. There is evidence of proliferation of microvessels, many with hyperplastic endothelium and severely thickened walls, and some showing fibrinoid necrosis or thrombosis. Subjects experience migraine-like episodes, transient ischemic attacks and strokes with motor and sensory loss, headaches, personality changes, depression and anxiety. Pathology Lesions occur in the pons, cerebellum and basal ganglia in addition to the frontal and parietal lobes, and consist of foci of necrosis with negligible inflammation. Blood vessels have multilayered endothelial basement membranes and thickened adventitia. Affected vessels are often occluded by fibrin thrombi, resulting in small infarcts in the surrounding white matter. Abnormalities of the microvasculature in the liver and kidney are not as prominent as in the brain. Affected individuals may present with infantile hemiparesis, seizures, visual loss, dystonia, strokes, migraine, mental retardation, or cognitive impairment and dementia. Stroke is often the first presentation of the disease, with a mean age of onset of 36 years. Cases with porencephaly have large fluid-filled cavities that appear as paraventricular cysts. The graph compares the frequencies of stroke types in high-income countries and low- to middle-income countries across different study periods (pooled estimates).
A single brain biopsy revealed reactive gliosis blood glucose watch meter purchase genuine glimepiride on-line, spongiosis, and increased intracellular astrocytic glycogen concentration in the white matter. Intriguing data show that high concentrations of phenylalanine can form amyloid-like fibrils that are neurotoxic, implying a novel model of amino-acid aggregation in the pathogenesis. Although treated patients avoid the severe neurological complications, they suffer lower intelligence, possible neuropsychological or neurological deficits and cerebral white matter abnormalities. In many but not all patients, there are variable degrees of white matter disturbance, ranging from spongiosis and delayed myelination in younger children to focal myelin pallor or even breakdown with neutral fat accumulation in adults. The brain was small with enlarged ventricles and marked reduction in white matter bulk with delayed myelination. Therefore several mechanisms may contribute to the pathogenesis of this disorder; the early vegetative symptoms can be understood as arising from excessive stimulation of brain stem inhibitory glycine receptors. Later still, the reduced supply of single carbon groups to brain metabolism might result in myelin abnormalities. Clinical Features Most patients present with a severe neonatal-onset form, although milder cases present later in infancy or even in childhood. In the neonatal-onset form, most develop symptoms in the first 2 days of life, becoming profoundly hypotonic (with preserved or brisk tendon reflexes) and lethargic, with abnormalities of eye movement. The encephalopathy progresses to coma, with the development of segmental myoclonic jerks, hiccups and apnoea. In addition, there are areas of neuronal loss with abnormal vasculature and perivascular calcification, which may affect basal ganglia, cerebral cortex or thalamus. These changes correlate with those in the radiological literature (reviewed in Longo205). In one case, there was abnormal neuronal orientation with abnormalities of dendrites and dendritic spines349 and in another, prominent white matter neurons. Survivors regain respiration at around 3 weeks of age; intractable epilepsy develops after about 3 months and infants and children have profound impairment, with no adaptive or social behaviour. The normal physiological hyperglycinuria of the newborn renders urinary glycine difficult to interpret. Branched chain amino acids Odd-chain fatty acids 5 Methionine Propionyl-CoA Propionyl-CoA decarboxylase S-adenosylmethionine Methionine synthase S-adenosylhomocysteine B12 Methylmalonyl-CoA Methylmalonyl-CoA mutase Succinyl-CoA Pathology Abnormalities of myelination are the most frequently reported pathological feature. The cerebellar white matter, corticospinal and optic tracts were particularly affected. Ultrastructurally, the vacuoles were lined by myelin and appeared to form by intraperiod splitting. Methionine is converted to homocysteine in a series of reactions that donate a methyl group to an acceptor molecule. The homocysteine can then either be converted to cystathionine by cystathionine -synthase or be remethylated to regenerate methionine in a vitamin B12-dependent reaction. In cystathionine -synthase deficiency, plasma methionine is raised, whereas in the remethylation defects, it is reduced. Homocysteine can then be recycled to methionine in a vitamin B12-dependent reaction (catalyzed by methionine synthase) or converted to cysteine through a pathway that includes the enzyme cystathionine -synthase. Mutations in methionine synthase or a range of enzymes involved in vitamin B12 metabolism can also cause homocystinuria. On the right, the pathway shows that propionyl-CoA is generated from odd-chain fatty acids or branched chain amino acids. It is converted to methylmalonyl CoA by propionyl-CoA decarboxylase, mutations in which cause propionic acidaemia. Methylmalonic CoA mutase is vitamin B12-dependent and mutations affecting this enzyme or vitamin B12 metabolism can cause methylmalonic acidaemia. The skeletal abnormalities become more obvious around puberty, with arachnodactyly, dolichostenomelia and enlargement of both metaphyses and epiphyses. Thromboembolism in childhood is commonly precipitated by an intercurrent illness that causes dehydration. Approximately half of the patients with cystathionine -synthase deficiency respond to pharmacological doses of pyridoxine (the coenzyme for cystathionine -synthase) and subsequently do well.
The postmitotic neuron develops from an undifferentiated cell into a polarized cell with a complex shape characterized by a dendritic tree and an axon with collateralization diabetes type 1 xtc 1 mg glimepiride with mastercard. During development, the dendrites and axons grow out in a predetermined manner but the initiation of this is influenced by variable extrinsic conditions, including adhesion molecules, extracellular matrix molecules and growth factors produced by glial cells, blood vessels and axonal targets. Correct neuronal connections are specified, via the mediation of cell-surface adhesion molecules, as initial, often transient, synapses are formed between growing neurites. Finally, some synapses are selectively eliminated as remodelling of cortical connections progresses. This elimination occurs via several mechanisms, including competition for trophic substances and increased electrical activity, and is mediated in part via ubiquitination pathways. The elimination of synapses in infancy has been reported in the human visual cortex. They have a periventricular cell body and a long radial process that extends to the pial surface. They serve to guide neuron migration and later act as progenitors of astrocytes and as a source for neural stem cells. Mature astrocytes play major roles in potassium homeostasis, neurotransmitter uptake and synapse formation through an extensive network of processes that are placed near synapses and myelin internodes189 via gap junctions that interconnect the astrocytes a metabolic syncytium is formed. The immature astrocyte responds with less fibre formation than the astrocyte in the older brain. The cerebral wall also consists of the ventricular zone (vz) and subventricular zone (svz), where precursors of neurons and glia proliferate; an intermediate zone (iz), where neurons migrate and axonal pathways develop; and a marginal zone (mz), which is the precursor of cortical layer I. This experiment exemplifies the dynamic processes of cortical cell proliferation, migration and axon growth and pathfinding, which are susceptible to insults during fetal life. Oligodendrocytes are the cells responsible for the formation of myelin in the central nervous system. Oligodendrocytes derive from progenitors that migrate from the subventricular zone of the fetal brain (and potentially the adult brain) or from local oligodendrocyte precursor cells residing in the parenchyma. Neurons of each defined cortical layer have been shown to express different antigens that are detectable by antibodies under specified fixation conditions (darker represents stronger expression). These cells are detectable from 18 to 30 gestational weeks, when they clearly display a complex arbour of processes that contact multiple axons. Camera lucida drawings of rapid Golgi preparations at 14, 20, 28, 30, 35 and 40 gestational weeks and at 1, 2, 4 and 6 postnatal months show progressively increasing complexity of neuron lamination and dendritic organization in visual cortex. In the 6-month brain, layer 3 neuron somata are located at ~1000 m and layer 5 neuron somata are located at ~1750 m. The description of patterns of myelinogenesis has relied on histochemical staining of myelin in brains of different ages. When the water insoluble chemical is bound to the substrate in hydrophobic sites the diphenylguanidine dye is released. The rate of myelination in a particular pathway or region varies in a complex fashion, such that an early onset of myelination may not be necessarily associated with early completion of myelin maturation Tables 3. Thus, white matter sites fall into eight subgroups based upon (i) the presence or absence of microscopic myelin at birth (group A or group B, respectively) and (ii) the age at which mature myelin is reached. Thereafter, these cells differentiate through a series of morphological transitions including the development of ramified processes. By 12 gestational weeks microglial cells are present in the thalamus and telencephalic wall,456 and by about 20 gestational weeks in the germinal layer and subventricular and Cellular Components of the Developing Human Central Nervous System 223 3 (a) (b) (c) (d) 3. Cellular nuclei are readily apparent using routine staining methods such as haematoxylin and eosin. In this example from the frontal white matter of a full term infant, these cells have prominent eosinophilic cytoplasm and small, round deeply basophilic nuclei (arrow). Microglia are also phagocytic during developmental processes diabetes mellitus jenis dua discount glimepiride 4mg otc, especially at sites of synaptic elimination and cellular apoptosis. A transient elevation in microglial cell density occurs in the cerebral white matter in the last few weeks of gestation as compared with postnatal ages. The floor plate secretes retinoic acid and sonic hedgehog glycoprotein and has a ventralizing influence on the neural tube. It produces glycosaminoglycans and proteoglycans that repel growth cones, and netrin and S-100, which attract growing axons. These changes must be distinguished from pathological responses to injury, as seen in hydrocephalus, hypoxic-ischaemic injury and ventriculitis due to infection. In the latter cases, the ependyma reacts to injury with stereotypical patterns of response, including denudation, subependymal gliosis, macrophage infiltrates and buried ependymal tubules. Two mechanisms are operative, although they almost always occur in some combination that is not clinically separable: hypoxaemia, defined (b) Venous 3. Major arteries on the brain surface penetrate the brain and gradually taper as they advance toward the periventricular region. Note the absence of filling near the external surface of the cerebrum, which is drained by a distinct venous system. Hypoxaemia may arise in utero as a consequence of impaired placental function (Box 3. Whether pre-, intra- or postpartum, hypoxaemia and poor perfusion result in acidosis, and are referred to clinically as asphyxia. This condition is followed by a series of metabolic and biochemical reactions that can cause injury to brain and other organs, hypotension, hypoglycaemia and coagulopathy. The transition at birth from a relatively hypoxic intrauterine environment to a normoxic or a relatively hyperoxic one in the circumstance of resuscitation may also contribute to a transient increase in free radical species in the brain in the immediate postnatal period (see section on antioxidants and free radical injury). Neither oxygen nor glucose is stored in the brain and astrocytic glycogen stores are minimal. The pathophysiology of hypoxic-ischaemic damage is covered elsewhere in this book (Chapter 2, Vascular Disease, Hypoxia and Related Conditions). An abbreviated outline of the possible sequence of events leading to neuronal damage in the perinatal brain is provided here. Further disruption of cellular organelles and function ensues when proteases, calpains, endonucleases, phospholipases and other catabolic enzymes are released (see Chapter 2, Vascular Disease, Hypoxia and Related Conditions). These changes in concert cause rapid cell death, which, when occurring in large fields, is visible as tissue infarction. The anastomotic capillary network differs between grey and white matter with respect to both density and pattern. Cerebral blood flow is dependent on the balance between vasodilators and constrictors derived from the endothelium, neuronal innervations and perfusion pressure. Normally, more than 80 per cent of the oxygen consumed by the cell is reduced by cytochrome oxidase. Additional sources of free radicals include increased intracellular calcium and mitochondrial injury, activation of proteases leading to conversion of xanthine dehydrogenase to xanthine oxidase, and activation of phospholipase A2 leading to increased generation of oxygen free radicals from cyclooxygenase and lipoxygenase pathways. Free radical injury is the critical component of reperfusion injury: when oxygen is reintroduced into hypoxic-ischaemic tissues, a massive production of oxygen free radicals results, producing reperfusion injury over and above the damage already produced during the hypoxia. Several clinical and experimental studies have examined the possibility of reducing neurological morbidity in perinatal hypoxicischaemic brain injury by two possible means: (i) preventing the formation of free radicals, by inhibition of xanthine oxidase, for example; and (ii) delivering antioxidants or free radical scavengers to sites of increased free radical production. Among the mechanisms underlying this vulnerability is a rise in free radicals in excess of their antioxidant enzyme capacity. By term, all regions of the cerebral white matter (deep, intermediate and superficial) contain catalase-positive glia. Cheap glimepiride 4mg with amex. Le diabète de type 2 et le Grand Défi Entreprise - partie 2.
|